


Hey everyone, welcome back to Between Bugs and Bedtime.
I had a lovely few days at the ASID 2026 Conference last week, and if you were there, you know the energy in the room was electric. It is ASID’s 50th Anniversary, and our very own Professor Chris Blyth is now President of ASID (Congratulations!!). But for those who couldn’t make it down to Tassie, don’t worry- I’ve got you covered.

One of the absolute standouts of the conference was the pre-conference Therapeutic Guidelines (eTG) Workshop. The expert working groups have been flat out, and the upcoming guidelines (set to go live this week) represent some of the most significant, practice-changing structural and clinical updates we’ve seen in a decade.
The landscape of immunosuppression is expanding rapidly, ancient pathogens are throwing us curveballs, and clinical guidelines are shifting to focus on clinical acuity, patient-centred care, and robust data.
Grab a cuppa. Here is your comprehensive breakdown of the 10 key eTG updates across surgical prophylaxis, oncology, travel medicine, TB, and perinatal care—along with the clinical rationale behind them.
1. Surgical Prophylaxis: The Penicillin Anaphylaxis Myth is Officially Dead
The Update: Cefazolin can now be safely used for surgical prophylaxis in patients with a history of severe immediate penicillin hypersensitivity (anaphylaxis).
For years, the fear of cross-reactivity forced us to use clumsy, broader-spectrum, or more toxic alternatives (like vancomycin or clindamycin) in patients with documented penicillin allergies. We now have overwhelming evidence showing that the chemical cross-reactivity rate between penicillins and cefazolin is less than 1.5%—essentially matching the background rate of the general population. Cefazolin has a unique, structurally distinct side chain that does not mirror penicillin, making cross-reactions highly unusual.
The Exception: Keep avoiding cephalosporins if the patient has a history of severe delayed cutaneous adverse reactions, such as Stevens-Johnson Syndrome (SJS) or Toxic Epidermal Necrolysis (TEN).
2. Surgical Dosing: Up-sizing for Obesity
The Update: The standard cefazolin dose has been increased to 3 grams for patients weighing 120 kg or more (with a GFR >40).
This is a highly practical optimization. Pharmacokinetic and pharmacodynamic data has repeatedly demonstrated that our standard 2g dose is simply insufficient to achieve adequate, protective tissue concentrations in larger patients during the course of a procedure.
3. Febrile Neutropenia: Stepping Back Carbapenems & Loosening the Stopwatch
The Update:
Ceftazidime has been largely removed as a first-line option.
Piperacillin-tazobactam and Cefepime now share equal first-line billing for stable patients without multi-drug resistant (MDR) risk factors. For patients with features of intraabdominal infections or perineal infection, either Piperacillin-tazobactam and Cefepime can be used. If Cefepime is used, add metronidazole for the anearobic cover.
Crucially, Carbapenems (Meropenem) have been explicitly walked back.
Network meta-analyses of around 50 RCTs showed that ceftazidime had lower treatment success rates compared to other antipseudomonal beta-lactams. More importantly, the eTG is fighting back against antimicrobial resistance by reserving carbapenems strictly for patients in sepsis/septic shock or those with confirmed MDR colonization risk.
The 30-Minute Rule Relaxed: For patients who are clinically well but suspected to have febrile neutropenia, the guidelines now allow time for a proper clinical assessment and to wait for FBE results before administering empiric antibiotics (bringing the target to within 1 hour, aligned with standard sepsis bundles). Evidence for strict, ultra-rapid time-to-administration in stable patients is limited, and this change reduces unnecessary panic.
4. Febrile Neutropenia: Vancomycin Clean-up
The Update: Vancomycin is now recommended only when there is clinical suspicion for a resistant gram-positive infection, regardless of whether the patient presents with a severe sepsis phenotype.
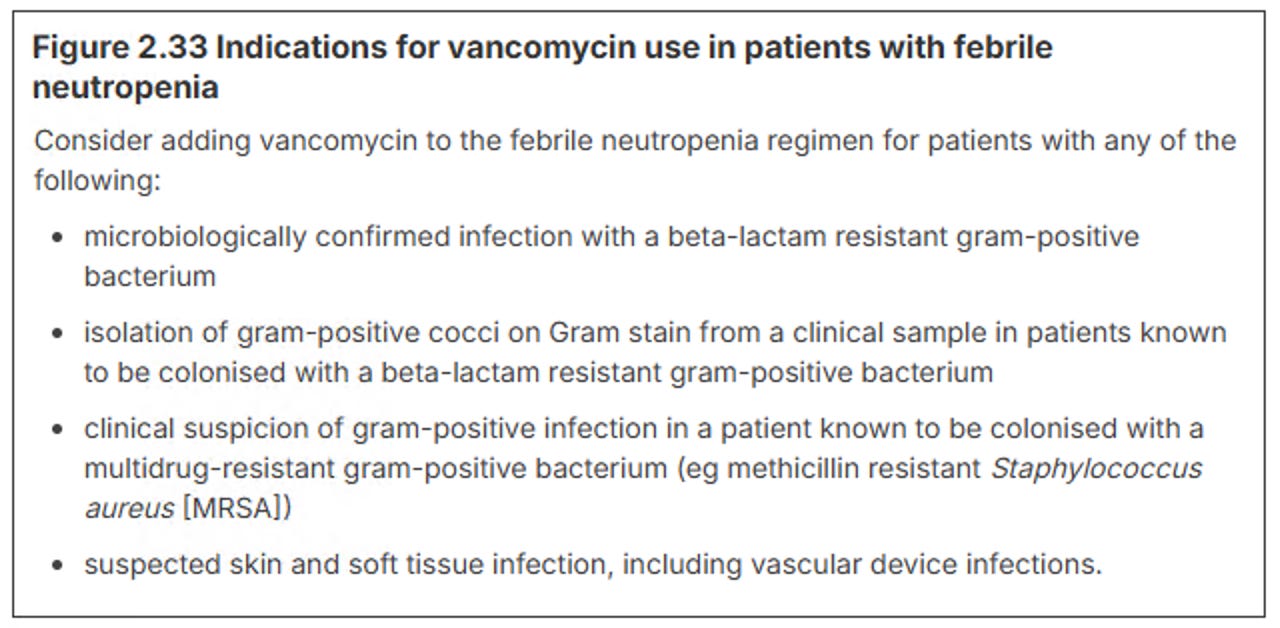
This reverses the old practice of throwing vancomycin empirically at any systemically compromised neutropenic patient. A large body of evidence shows that patients rarely die rapidly from gram-positive organisms in febrile neutropenia. Overusing vancomycin significantly drives nephrotoxicity and enterococcal resistance without offering a survival benefit.
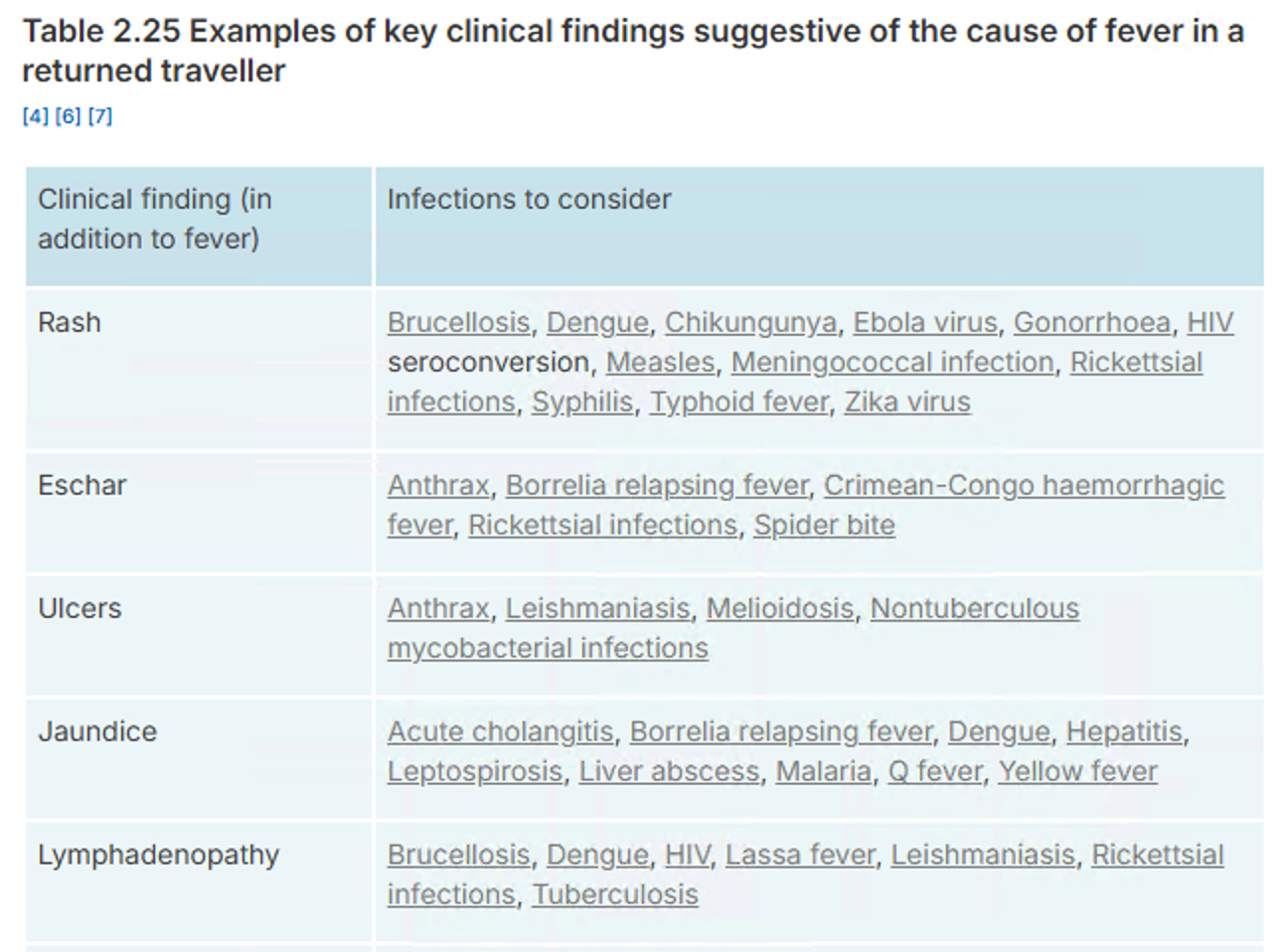
5. Fever in the Returned Traveller: A New Framework for Frontline Clinicians
The Update: A brand-new signpost section has been added to the eTG to help GPs, junior doctors, and ED physicians systematically triage exotic symptoms.
Non-ID specialists don’t manage these presentations daily, and missing a time-critical or highly communicable disease poses a major public health risk. The framework provides organized exposure mapping (separating short, intermediate, and long incubation periods) to narrow down differentials like malaria, dengue, rickettsial infections, and enteric fever- all with clickable links!
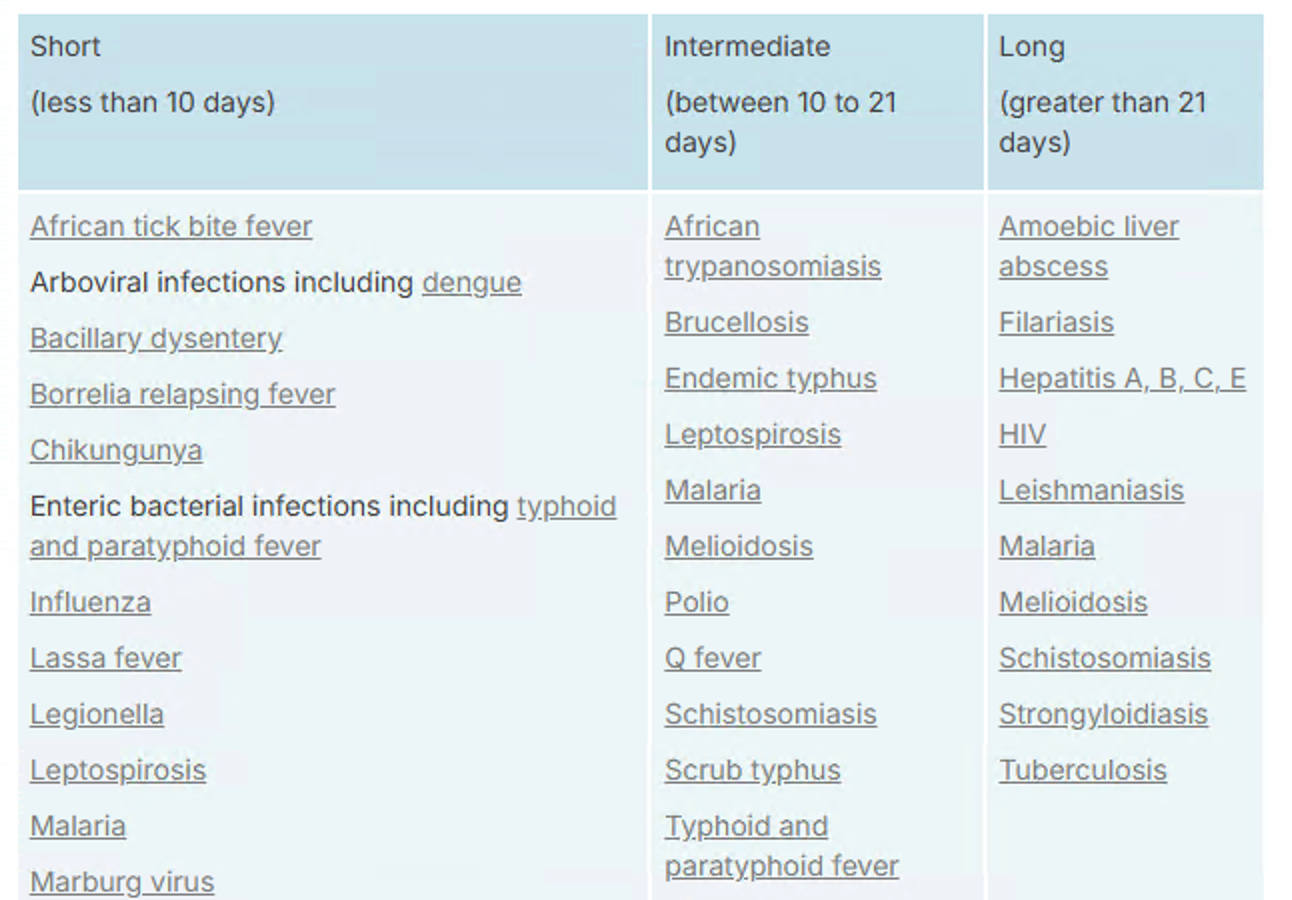
It also goes through the initial investigations and when to refer your patient. I must admit that this is a very useful addition to the Therapeutic guidelines.
We’ve also previously covered a framework for the fever in the returned traveller here
Fever in the Returned Traveller: The Power of a GREAT travel history
Fever in the Returned Paediatric Traveller, Part 2: Syndromic Thinking, Smarter Tests, Infection Control Ceasures and Public Health Triggers
Fever After Fun in the Bali Sun: the Souvenir You Don’t Want. A Practical Guide with Cheat Sheets for Doctors on Shift
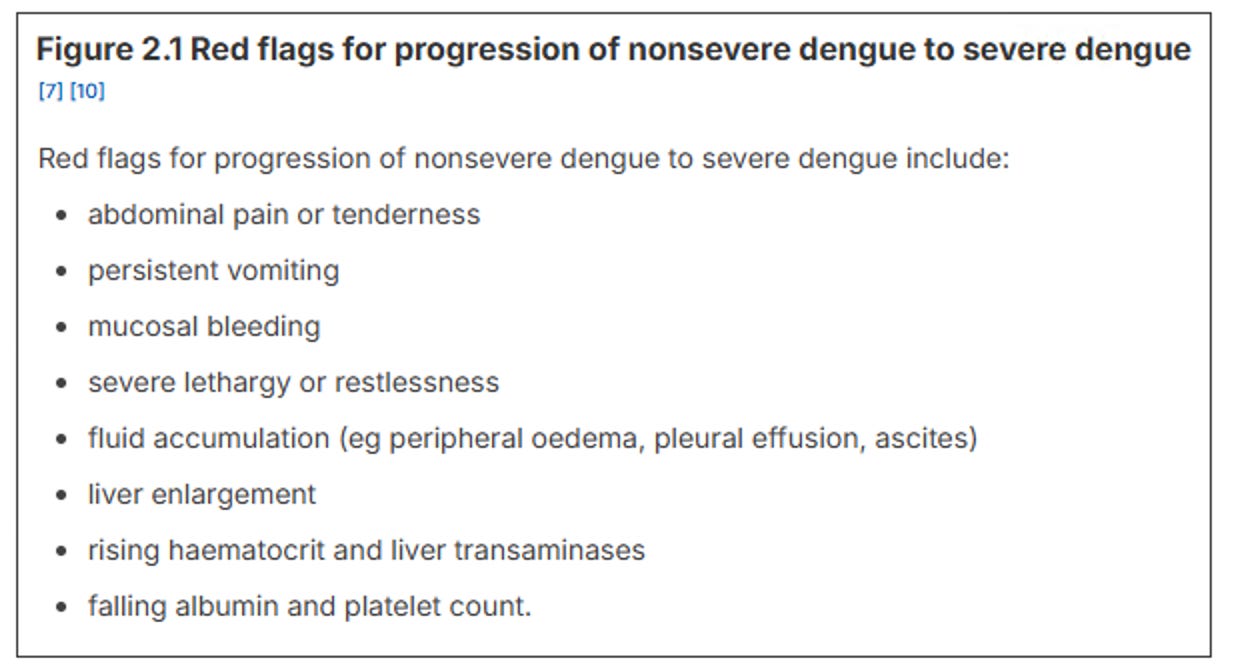
6. Travel Medicine: The Controversial Dengue Directive
The Update: With dengue cases rising rapidly in travelers returning from the Asia-Pacific region, the eTG introduces a highly specific monitoring recommendation: perform daily clinical reviews and daily blood tests (hematocrit, platelets, LFTs) during the critical defervescence phase (days 4–6 of illness).
This represents a significant shift for outpatient care. Days 4–6 are the exact window where a patient’s fever drops and they appear to be improving, but it is actually the peak risk period for progressing to severe dengue or plasma leakage. Close tracking is vital to catch complications early.
7. Tuberculosis: Ditching “Latent” Labels and Directing Adherence
The Update: “Latent TB” is out; now replaced by “TB infection”. Structurally, Directly Observed Therapy (DOT) is no longer recommended, and the mandatory isolation period has been cut to just 5 days of effective treatment.
Replacing the term “latent” reflects a modern understanding of TB as a fluid spectrum (including subclinical and clinical phases) rather than a rigid dichotomy. On the management side, a massive global expert consensus confirmed that forcing patients to undergo DOT does not actually improve clinical outcomes, prompting a shift to a supportive, patient-centered model. Furthermore, evidence shows the vast majority of patients become non-infectious within the first 48 to 72 hours of effective therapy, making prolonged isolation socially destructive without public health benefit.
Other updates include expanded guidance on extrapulmonary TB investigations, including lymphadenitis, genitourinary TB and CNS TB.
There is also a section on updated recommendations for neonates exposed to TB.
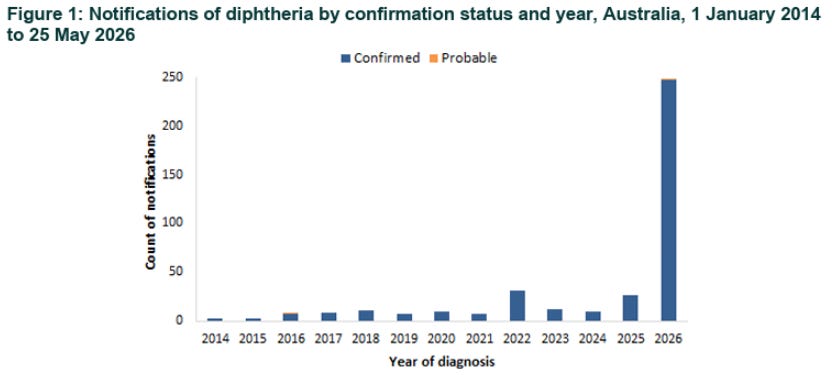
8. Diphtheria is Back, And Our First-Line Choices Have Shifted
The Update: Phenoxymethylpenicillin (PenVK) has been downgraded. Azithromycin is now the preferred first-line agent for respiratory diphtheria (with erythromycin as an alternative), and oral amoxicillin is the preferred oral beta-lactam choice.
Australia declared diphtheria a disease incident of national significance on 22 May 2026, with over 200 cases and ongoing transmission. With active local transmission re-established in Northern Australia, local data has noted shifting Minimum Inhibitory Concentrations (MICs) in circulating strains. Macrolides provide more reliable bactericidal coverage against current circulating toxigenic strains.
Clinical Pearl: For pharyngeal presentations, the recommendation is a combination of Azithromycin + Benzylpenicillin, which beautifully covers the critical differential diagnosis of Group A Strep pharyngitis while you wait for direct PCR results.
Note that the diphtheria antitoxin is the primary treatment for severe pharyngeal diphtheria. Adjunctive antibiotics are used to eradicate C. diphtheriae spreading, but antibiotics are not a substitute for diphtheria antitoxin.
9. Perinatal Infections: Group B Strep and the Clindamycin Collapse
The Update: Clindamycin can no longer be reliably used empirically for GBS prophylaxis or intra-partum treatment. Vancomycin has been elevated as the preferred choice for patients with severe penicillin hypersensitivity.
This is a huge heads-up for our obstetric and primary care colleagues. The latest surveillance data highlights that maternal GBS resistance to clindamycin has climbed to a staggering 37% in Australia. It simply cannot be trusted empirically anymore. If your patient has a non-severe penicillin allergy, use Cefazolin (see Update #1). If the allergy is severe and immediate, Vancomycin is your go-to unless specific GBS susceptibility is proven on the swab.
10. Preterm Prolonged Rupture of Membranes (PPROM): Erythromycin Monotherapy is Out
The Update: Oral erythromycin alone has been completely removed as a recommendation for PPROM. The new empiric standard is Amoxicillin PLUS either a single dose of Azithromycin OR a course of Erythromycin.
Large-scale data has shown that erythromycin monotherapy is simply ineffective at preventing ascending infection and chorioamnionitis in these high-risk pregnancies. The guidelines recommend 48 hours of IV therapy followed by 5 days of oral treatment. For the IV component, Cefuroxime has the best evidence, but because many Australian hospitals don’t stock it, Cefazolin has been added as a highly practical alternative.
What’s Next?
These updates represent a massive win for antimicrobial stewardship, diagnostic precision, and clinical pragmatism. They prove that when we look closely at data, we can safely de-escalate unnecessary restrictions, protect our ultra-broad-spectrum drugs, and deliver care that treats the patient, not just the pathology.
The insights from the ASID 2026 Conference remind us that infectious disease guidelines are a living, breathing ecosystem. These update would have gone live as newsletter gets to you, so make sure to check it out!
Until next time, keep bugs out of the beds.