



Cracking the Case: The Paediatric Infectious Disease History Taking
A practical guide to asking the right questions—because every fever has a backstory, and great ID care starts with a great history

Taking a medical history in paediatrics is both an art and a science. Get it right, and you're often well on your way to the diagnosis – some estimate that up to 90% of paediatric diagnoses stem from a meticulous history. When infectious diseases are suspected, the stakes are even higher. Children, especially infants, can present with vague symptoms, communication relies heavily on caregivers, and subtle clues can signal serious illness.
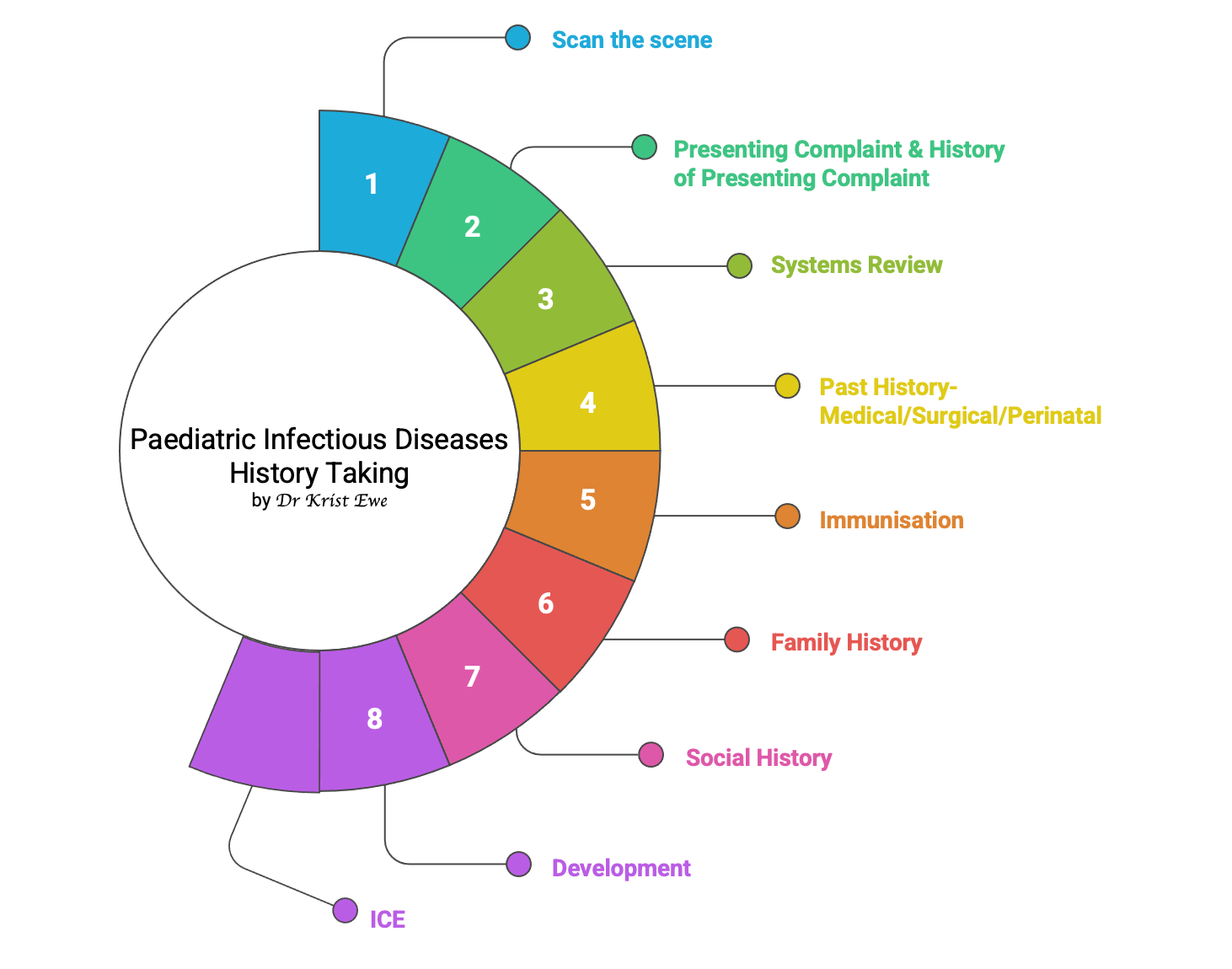
Mastering a structured yet adaptable approach is key. This isn't just about ticking boxes; it's about actively listening, building rapport , and applying an "infectious disease lens" to every piece of information gathered. In my experience, the ID team is often called upon to solve undiagnosed mysteries- because they tend to take meticulous histories. Here’s a framework (covers steps 1-3 of the 5-Step Infection Framework) to guide you, particularly when infection is on the cards:
Setting the Stage and Scanning the Scene
Start with the essentials: confirm the child's name, age, and who is with them. Introduce yourself clearly and explain your purpose. Creating a friendly, non-threatening environment is crucial, especially with younger children. Here you are already looking for clues in your interaction with the family unit, as well as looking for signs that will help you in your history taking.
Presenting Complaint (PC): The Starting Point
Use open-ended questions like, "What brought you in today?". Record the main problem in the parent's or child's own words. Note the primary symptom suggesting infection (e.g., fever, rash, cough).
History of Presenting Complaint (HPC): The Detective Work
This is where the deep dive happens. Get a chronological account (the timeline is key!) of the illness. For each symptom, explore:
Onset & Duration: When did it start? Sudden or gradual? How long has it lasted?
Character: What is it like? (e.g., barking cough, sandpaper rash, projectile vomit)
Severity: How bad is it? How does it affect activity, feeding, sleep, school/nursery? Use age-appropriate pain scales if needed.
Associated Symptoms: Fever (measured?), chills, aches, specific system symptoms (respiratory, GI, neuro)?
Timing/Pattern: Constant or intermittent? Worse at certain times?
Exacerbating/Relieving Factors: What makes it better or worse? Response to medication?
Previous Episodes: Happened before?
Crucially for Infections – The Exposure History:
Sick Contacts: Anyone ill at home, school, daycare? What symptoms? When?
Travel: Recent trips (where, when)? Activities? Prophylaxis? Bites? (more on travel history in another post)
Animals: Pets? Farm animals? Bites/scratches?
Environment/Food/Water: Daycare/school? Recent meals out? Undercooked food? Water source? Swimming? Tick exposure?
Systems Review: Casting a Wider Net
Briefly screen other systems for related symptoms. Key areas for infection include:
General: Fever, lethargy, irritability, appetite changes.
Respiratory: Cough, work of breathing, noisy breathing.
GI: Vomiting, diarrhoea, abdominal pain, urine output (wet nappies).
Neuro: Headache, seizures, altered mental state, stiff neck.
Skin: Rashes, sores.
Past Medical History (PMH): The Background Check
Previous conditions (esp. asthma, immunodeficiency).
Significant past infections, hospitalisations, surgeries (esp. splenectomy).
Perinatal History: Critical for Neonates and Infants
This period holds vital clues for early-life infections. Ask about:
Maternal Health: Infections during pregnancy (GBS status, TORCH/SCORTCH screens, STIs- chlamydia/ gonorrhea/ syphilis, fevers/rashes)? GBS treatment during labour? Medications? All serology (HIV, HepB, HepC, Syphilis, Rubella etc) and ultrasound results are relevant). Colonisation with multidrug-resistant organisms or hospitalisation in a different state or country can be relevant.
Labour/Delivery: Prematurity? Prolonged rupture of membranes (>18hrs)? Mode of delivery? Maternal fever during labour?
Neonate's Course: Birth weight? Apgars? Resuscitation needed? NICU stay? Early signs like temperature instability, feeding issues, respiratory distress, jaundice, lethargy? Sepsis workup or antibiotics given?
Immunisations: A Key Defence
Are they up-to-date? Confirm with the record (physical or electronic records or from the immunisation registry) if possible. Missed vaccines are a major risk factor.
Also, please remember additional vaccines and travel vaccines. Homeopathic vaccinations are not really vaccinations- there are guidance on these.
It’s worth noting that vaccination schedules are different for individual countries. Hence, “up-to-date” vaccinations in one country may not apply to another.
Development: Any Red Flags?
Are milestones appropriate for age? Significant delays can sometimes follow congenital infections.
Drug History & Allergies: What Are They Taking?
List all medications (prescribed, over-the-counter). Note recent antibiotic use and doses (could they be underdosed?). Any other intentional or accidental substance use or ingestion? Document allergies and type of reactions (especially to antibiotics).
Family History (FH): Looking for Links
Recent similar symptoms in contacts?
History of immunodeficiency or recurrent infections?
Consanguinity? We’re thinking primary immunodeficiencies here.
Social History (SH): The Environment
Who lives at home? Daycare/school attendance (high transmission risk)?
Household smoking (increases respiratory risk)?
Pets? This include pythons, rats, worms, turtles, etc.
For adolescents: Use HEEADSSS framework, focusing on substance use and sexual health if relevant.
Anyone else visiting from interstate or overseas?
Ideas, Concerns, Expectations (ICE): The Parent/Patient Perspective
What do they think is wrong? What are they worried about? What do they hope you can do? Addressing ICE builds trust and helps manage expectations (e.g., regarding antibiotics).
Putting It All Together
This framework provides structure, but flexibility is key. Build rapport, listen actively, and don't be afraid to deviate to follow important clues. Summarise periodically to check understanding. Remember pertinent negatives – documenting the absence of key signs/symptoms is diagnostically useful.
Taking a thorough, infection-focused history is a skill that develops with practice. By using a systematic approach combined with targeted questioning and active listening, you'll be better equipped to unravel the complexities of paediatric infectious diseases and provide the best possible care for your young patients
If you wish to learn something, let me know in the comments! Will try my best to cater to your learning!